|
|
Silicone Embolism Syndrome
Submitted by Joshua Clayton, MD
General Considerations
- Occurs following injection of liquid silicone, commonly for cosmetic purposes (most often young women and transgender females) due to low cost compared to plastic surgery
- Performed by unlicensed individuals at “pumping parties”
- Incidence unknown secondary to its illegal use by non-professionals
Pathophysiology
- Four types of histologic patterns have been seen
- Embolic
- Congestive
- Pneumonitis, and
- Diffuse alveolar damage
- Damage thought to be related to both mechanical obstruction of capillaries as well as activation of coagulation cascade following uptake by alveolar macrophages
- Silicone previously thought to be inert but recent evidence suggests silicone sensitivity in certain individuals following repeated exposure
Clinical Findings
- Similar to those of fat embolism, with vast majority of patients meeting the Criteria of Schonfeld for fat embolism syndrome
- Most commonly presents with predominantly respiratory symptoms
- Hypoxemia
- Dyspnea
- Fever
- Alveolar hemorrhage
- Neurologic involvement occurs in a smaller subset of individuals, uniformly fatal in documented cases
Imaging Findings
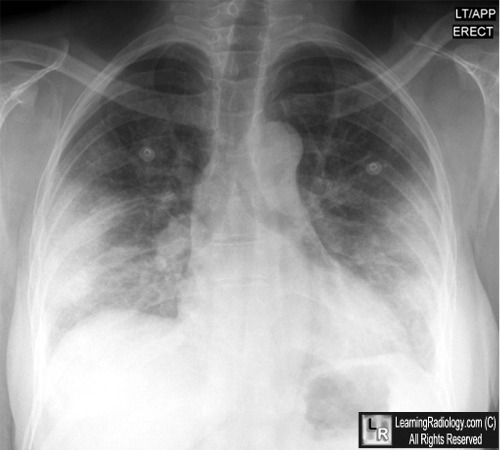
- Chest X-Ray
- Bilateral, diffuse alveolar opacities
- Parenchymal consolidation
- CT
- Ground glass opacities
- Peripheral distribution in over half of cases
- Less commonly, interlobular septal thickening or consolidation
Differential Diagnoses
- Acute alveolar disease
- Pulmonary edema
- Fat embolism
- Heart disease
- Adult respiratory distress syndrome (ARDS)
- Amniotic fluid embolism
- Neurogenic or High altitude pulmonary edema
- Diffuse alveolar hemorrhage
- Atypical pneumonia
- Pneumocystis (PJP, PCP)
- Cytomegalovirus (CMV)
- Herpes simplex virus (HSV)
- Respiratory syncytial virus bronchiolitis (RSV)
- Chronic interstitial disease
- Hypersensitivity pneumonitis (HP)
- Desquamative interstitial pneumonia (DIP)
- Nonspecific interstitial pneumonia (NSIP)
- Respiratory bronchiolitis interstitial lung disease (RBILD)
- Lymphocytic interstitial pneumonia (LIP)
- Sarcoidosis
- Pulmonary alveolar proteinosis (PAP)
- Drug toxicity
- Bronchiolitis obliterans with organizing pneumonia (BOOP, COP)
- Bronchoalveolar carcinoma
Treatment
- Supportive
- Supplemental oxygen
- Steroids
- Intubation if respiratory status indicates
Prognosis
- Overall mortality ~25%
- <10% with no neurologic involvement
- Approaching 100% with neurologic involvement
 
Silicone Embolism Syndrome. White arrows point to dense, peripherally located airspace disease which is
documented on axial and coronal reformatted CT scans of the chest (blue arrows).
For more information, click on the link if you see this icon 
For these same photos without the annotations, click here and here
Schmid, MD Tzur, MD, Leshko, MD Krieger, MD,FCCP; Silicone Embolism Syndrome
A Case Report, Review of the Literature, and Comparison With Fat Embolism Syndrome. CHEST June 2005 vol. 127 no. 6 2276-2281
Bartsich, Wu; Silicon emboli syndrome: A Sequela of clandestine liquid silicone injections. A case report and review of the literature. Journal of Plastic, Reconstructive & Aesthetic Surgery January 2010 Volume 63, Issue 1 Pages e1-e3
R. M. Goldblum MD, Corresponding Author Contact Information, A. A. O'Donell MD, Prof D. Pyron MTa, R. M. Goldblumb, R. P. Pelley MDc, A. A. O'Donelld and Prof J. P. Heggers PhD; Antibodies to silicone elastomers and reactions to ventriculoperitoneal shunts. The Lancet Volume 340, Issue 8818, 29 August 1992, Pages 510-513
Restrepo CS, Artunduaga M, Carrillo JA, et al. Silicone pulmonary embolism: report of 10 cases and review of the literature. J Comput Assist Tomogr. Mar-Apr 2009;33(2):233-7
Chung KY, Kim SH, Choi YS, et al. Clinicopathologic review of pulmonary silicone embolism with special emphasis on the resultant histologic diversity in the lung e a review of five cases.Yonsei Med J 2002;43:152e9.
Shah, Rosita and Wallace Miller, Jr. Isolated Diffuse Ground-Glass Opacity in Thoracic CT: Causes and Clinical Presentations. AJR 2005; 184:613-622
|
|
|

{kind=link}
{kind=link}